
This toolbox, developed by IAS – the International AIDS Society, together with partners, is designed as a rapidly deployable resource to support national governments in responding to unexpected reductions in HIV funding by enabling swift reassessment and reorganization of HIV systems and services.
Version: 4 December 2025



The TIER Tool – Tool for Intervention, Evaluation and Ranking (IAS) (Version 30 July 2025)
This tool offers a structured framework for prioritizing components of an HIV programme, including HIV treatment and care (continuity, monitoring, initiation and re-initiation), testing and prevention. It incorporates adaptable prioritization criteria according to the epidemiological context and progress toward the 95-95-95 targets.
French – Lʼoutil TIER dʼévaluation et de classement des interventions (IAS) (Version 30 juillet 2025)
Spanish – La herramienta de evaluación y clasificación de intervenciones (TIER) (IAS) (Versión del 30 de julio de 2025)
Portuguese – TIER – Ferramenta de Avaliação e Classificação de Intervenções (IAS) (Versão de 30 de julho de 2025)
Key questions
- Who is represented in the technical working group responsible for developing the prioritized list or tiers of HIV services?
- Does the group include HIV technical experts across the full cascade of services and populations currently served?
- Are civil society and community representatives meaningfully included in the process?
- Is there representation from planning and policy departments, and the Ministry of Finance, to ensure alignment with funding and broader health system considerations?
- Situational analysis: Is current analysis of the countries HIV response available with disaggregated data by age, sex and geography?
- Essential data includes:
- Cascade analysis
- Incident HIV acquisitions
- Number of HIV and early infant diagnosis (EID) tests performed for diagnosis
- Number of HIV tests performed for pre-exposure prophylaxis (PrEP) service delivery
- Number on PrEP disaggregated by method and population
- Rate of initiation on PrEP
- Number on ART
- Initiations on ART
- Numbers of Laboratory investigations performed (including viral load (VL), Xpert MTB/Rif, CD4, lateral flow lipoarabinomannan (LAM), cryptococcal antigen (CRAG) other)
- Number of people on TPT
- Cost data for each element of the HIV service package
- Additional data
- Advanced HIV disease cascade data
- Re-engagement data
- Differentiated service delivery (DSD) related data – numbers in defined DSD models
- Essential data includes:
- Have the following domains been considered in the prioritization analysis?
- Epidemiological analysis
- Cost effectiveness and resource optimization
- Feasibility and health system readiness
- Ethical and equity considerations – across the health system
- Acceptability and community engagement
- Social and economic impact
- Has a model for prioritization been agreed upon?
- Number of tiers to be considered (Two- minimum and optimal services- or three tier model – minimum, standard and optimal)
- Has a comprehensive list of interventions/components of the service package been developed?
- Has a comprehensive assessment of all interventions/components of the service package been developed?
- Has, or can, modelling of the impact of the chosen prioritization model been performed; including an analysis of the costs versus the number of new acquisitions or deaths averted?
- Which programme elements are fully established at national level versus early roll out and piloting?
- How will any changes in the clinical and service delivery package be communicated to staff?
- How will any changes in the service package be communicated to recipients of care?
Tools and resources
Sustaining priority HIV, viral hepatitis and STI services in a changing funding landscape: operational guidance
World Health Organization, Pre-publication draft (July 2025)
More information on the Sustaining priority HIV, viral hepatitis and STI services in a changing funding landscape: operational guidance
The 2025 WHO operational guidance provides a structured approach to support countries in sustaining priority services for HIV, viral hepatitis and sexually transmitted infections in the context of reduced external funding. It proposes practical steps to assess risks, set priorities and adapt services and systems. The guidance introduces a step-wise priority-setting framework that organizes services into three tiers based on their contribution to achieving national and global health outcomes. Tier 1 is “essential” services, of Tier 2 is “important” and Tier 3 is the “extended” package. What is included in each of these tiers is context, population and resource specific. Supporting documents are available here.
The guidance also includes:
- key steps to assess and monitor service disruptions and health financing risks;
- a systematic process for setting priorities for services and interventions;
- cross-cutting enablers such as health workforce strategies, resilient supply chains, integrated data systems and inclusive governance;
- an emphasis on people-centred approaches and sustained community engagement to ensure that services remain accessible, acceptable and responsive to those most severely affected;
- opportunities for service integration, especially within primary health care, to enhance efficiency and sustainability; and
- strategic recommendations for financing transitions, including alignment with public financial management systems and domestic resource mobilization.
The TIER tool – Tool for Intervention Evaluation and Ranking
IAS, 2025. An HIV service package prioritization tool
More information on The TIER tool
This tool is designed to support countries in their planning and prioritization of HIV programme elements in the context of funding shifts. It provides a structured framework to prioritize HIV programme components – across testing, treatment, and prevention – based on epidemiological context and progress towards the 95-95-95 targets.
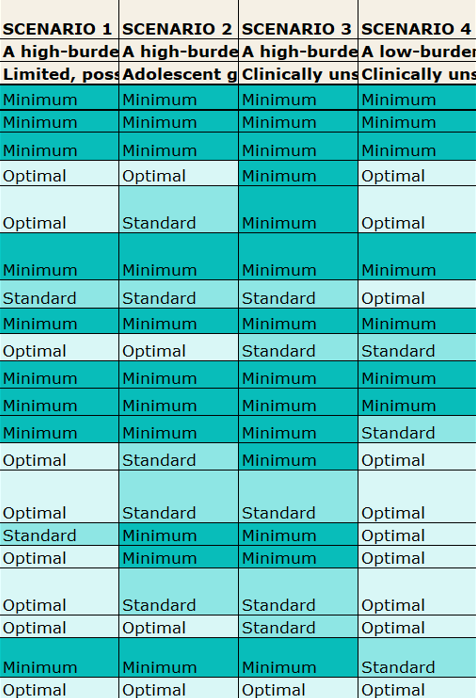
The tool uses illustrative examples of prioritization across four scenarios:
- A high-burden country achieving 95-95-95 targets across all populations
- A high-burden country achieving the targets but not across all populations
- A high-burden country not yet achieving one or more of the 95-95-95 targets
- A low-burden country not yet achieving one or more of the 95-95-95 targets.
For each scenario, a suggested prioritized list of interventions is provided across key programme areas. Users can select the scenario most relevant to their context, and then adapt, review and adjust the priorities noting the rationale for the decisions made.
Interventions are prioritized into three illustrative tiers:
- Minimum – Services that are critical to maintain for continuity of care and health outcomes
- Standard – Important to sustain; should be reassessed frequently for continuation as funding allows
- Optimal – To be supported when additional resources are secured or efficiencies gained.
In addition, interventions can also be flagged as “not applicable” or to “discontinue”. More or fewer tiers could be considered. The relevant WHO guidelines are also provided alongside each intervention.
Outputs from the tool can inform modelling analyses to assess the projected impact of different prioritization approaches on new acquisitions and mortality. It can also support budgeting exercises by estimating resource needs for each tier, helping programmes plan for phased service expansion as funding allows.
GC7 Programmatic Reprioritization Approach: Protecting and enabling access to lifesaving services
The Global Fund to Fight HIV, TB and Malaria, version 10 June
More information on the GC7 Programmatic Reprioritization Approach
This new guidance supports Country Coordinating Mechanisms (CCMs) and Principal Recipients (PRs) in reprioritizing interventions to maximize impact under constrained funding. The guidance emphasizes that reprioritization should be tailored to each country’s context, taking into account programmatic interdependencies and all available funding sources. It also aims to prepare for Grant Cycle 8 (GC8) by promoting integration, cost-effectiveness, and sustainability of HIV, TB, and malaria programs within primary health care and community systems. Initial steps have included pausing or deferring lower-priority activities to reallocate resources toward critical, lifesaving services.
For HIV-specific interventions, the recommendations outline three priorities.
- Priority 1 focuses on saving lives through the procurement and delivery of antiretroviral therapy, support for treatment continuation, ART cohort expansion and management of TB and advanced HIV disease.
- Priority 2 emphasizes identifying people living with HIV who are not yet on treatment and linking them to care, using cost-effective testing strategies targeted at high-risk populations and settings.
- Priority 3 aims to protect primary prevention efforts, including condom distribution, PEP, PrEP for current users and new users in high incidence locations and/or people at increased risk, and harm reduction services.
Cross-cutting considerations include support to human resources for health, data and laboratory systems, addressing barriers to access, and implementing integrated health and community systems interventions to enhance efficiency and sustainability of HIV programs.
This guidance is also now available in French, Portuguese and Spanish.
More information on The Goals HIV epidemic model
The Goals HIV epidemic model is a tool where the amount and the allocation of funding to HIV interventions can be shifted within the model and show the impact on national goals, such as reductions in new HIV acquisitions or AIDS deaths. Goals is part of the Spectrum software suite most countries use to prepare their national HIV estimates. Goals modeling can help inform national decision-making by examining the impact, cost, and cost-effectiveness of different components of the HIV program. Technical assistance is available from Avenir Health to apply the model in countries facing shifts in donor support.
Here is an example of a modelling analysis with contact information on the final slide.
Global Fund pooled procurement mechanism reference pricing resources
The links below provide benchmark pricing of HIV diagnostics and medications procured through the Global Fund’s pooled procurement mechanism. These reference prices can serve as target prices to inform national budget planning and price negotiations in both national and regional procurement.
Although cost effectiveness of interventions should be assessed for each context, immediate budget impact of continuing and stopping each intervention must be included in the analysis.
- The Global Fund, version April 2025, “Pooled Procurement Mechanism Reference Pricing: ARVs”
- The Global Fund, version April 2025, “Pooled Procurement Mechanisms Reference Pricing: Strategic medicines used in HIV programs”
- The Global Fund, version Q2 2025, “Pooled Procurement Mechanisms Reference Pricing: RDTs”
- The Global Fund, version October 2024, “Category and Product-level Procurement and Delivery Planning Guide – Health and non-health products”
- The Global Fund, 11 May 2020, “Pooled Procurement Mechanism Reference Pricing: Advanced HIV disease products”
Country examples
In February 2025, Malawi and Zambia published guidance on prioritized HIV service delivery package. Table 1 summarizes the national guidance describing key activities continued, adapted or stopped across the cascade of HIV care for each setting.
- Malawi Secretary for Health, 24 February 2025, “Updated guidance on provision of uninterrupted HIV services across all health facilities”
- Zambia, Prof Lloyd Mulenga, Director of Infectious Diseases, Ministry of Health, 24 April 2025, “Minimum package of HIV services” presented to the HIV Technical Working Group
Table 1: National guidance on prioritization of HIV services in response to funding cuts
| Treatment | Testing | Prevention | |
|---|---|---|---|
Malawi | Provide ART initiation and continuation Maximize 6-month ART dispensation for all stable and eligible patients Coordinate patient transfers between sites to balance workload. This must be done in close collaboration with the clients, sending and receiving facilities. Routine scheduled VL testing services; sites with capacity for sample collection, transportation, and result utilization. Targeted VL sample collection should be provided at all sites. Routine Advanced HIV Diseases (AHD) screening for all eligible patients (including TB) Continue provision of Cotrimoxazole Preventive Therapy (CPТ) and TB Preventive Therapy (ТРТ). Register all clients requiring emergency refill as transfer-in upon production of the health passport. Emergency ARV dispensing for unregistered clients remains suspended. Continue with HIV drug resistance monitoring through genotyping for eligible clients at all sites. Facilitate easy ART access for children and teens where feasible. | Provide testing services (HIV, Syphilis and Hepatitis B) for all populations at risk Provide VCT services for all eligible clients. Directly assisted self-testing and distribution of self-tests for partners of VCT clients and pregnant/breastfeeding women. Provide DNA-PCR Testing for HEI. At facilities with capacity for sample collection, transportation/processing and result utilization. Provide rapid HIV test for HEI at 12 months and 24 months all sites | Provide Infant HIV Prophylaxis (Nevirapine [NVP], 2P [Zidovudine/Lamivudine/Nevirapine], Cotrimoxazole [CPT]) at all sites. Distribute condoms in the facility and community using existing available community health workers Provide oral PrEP for new and continuing clients at existing PrEP sites with adequate staffing for testing and PrEP provision. Provide injectable PrEP to continuing clients at existing Path-to-Scale facilities, with new initiations limited to pregnant and breastfeeding women. VMMC services: Provide the service where there is capacity for trained staff, space, and commodities and does not interfere with routine service provision |
| Zambia | Stop generalized testing. Stop community follow up of index testing. Stop HIVST. Stop recency testing. | Provide VMMC, PrEP, PEP only at the facility If distributed in any community point, then this community point needs to be led by MoH, not IP and location should not incur rent. No stand-alone DREAMS or wellness facility. Prevention of mother-to-child transmission: no birth testing and no community follow up. | No priority for repeat TPT Complete drug resistance testing only after treatment failure. Provide Septrin prophylaxis only for PBFW and children. |
Other countries released guidance on emergency actions or mitigation plans to ensure uninterrupted services in the first half of 2025. These memos and circulars are accessible below:
- Cameroon, General Secretary, Ministry of Public Health, 4 February 2025, “CAMPSAR: Cameroon Mitigation Plan for Sustained AIDS Response following the USAID/PEPFAR’s Suspension”
- Mozambique, Ministry of Health, 11 June 2025, National Directorate of Public Health, Mitigation measures in the context of the suspension of external support and emergency situations in the response to HIV/AIDS
- South Africa, Director General of Health, 11 February 2025, “Provision of uninterrupted HIV services across all health facilities”
- Uganda, Office of the Permanent Secretary, Ministry of Health, 7 February 2025, “Guidance on improvement of service delivery in both central and local government health facilities”
Mozambique
The key points, a summary and the outcomes across the HIV care cascade from Mozambique’s strategic prioritization of HIV services exercise are outlined below.
Key points from Mozambique’s prioritization exercise
- Prioritization exercise presented as an iterative process that can be adapted to budgetary changes
- Budget data on commodities and distribution of costs across programmes was gathered in advance of the meeting.
- The TIER tool intervention list was adapted to align with national HIV guidelines.
- All stakeholders including Ministry and health representatives met in a single group rather than splitting into prevention, testing and treatment sub-groups.
Summary:
- 95% of Mozambique’s HIV programme funding comes from external donors. The Ministry of Health and Stakeholders viewed the prioritization exercise as iterative ongoing, adjusting to updates in funding availability.
- The exercise excluded human resource and systems costs.
- The Ministry of Health collected consumption and budget allocation data for medicines and other consumables of the program prior to the workshop, and participants viewed this information as essential for informed decision making.
- Before the meeting, the Ministry determined budget distribution based on the 2022 National AIDS Spending Assessment (NASA): 50% for care and treatment, 20% for testing, and 17% for HIV prevention.
- The group reviewed WHO recommendations within the TIER tool and compared them against national policies, then adapted the TIER tool to reflect the current suite of interventions.
- Participants modelled three funding scenarios using the adapted tool: 0%, 30%, and 70% of current external funding levels.
- The Ministry held a one-day internal technical working group (TWG) meeting to review the prioritization plan.
- A two-day multi-stakeholder workshop brought together civil society, donors, and implementing partners from across prevention, testing, and care and treatment.
- Experts from all programme areas jointly reviewed each section of the TIER tool. The exercise was intentionally completed together so every group understood understand the rationale and the results of the de-prioritization across the cascade.
Table 2: Mozambique’s prioritization outcomes across the cascade
| Testing | Prevention | Treatment |
| Prioritize testing and redefine eligibility criteriaCommunity-based testing was de-prioritized. HIV testing integrated into family planning services stopped. | Most prevention interventions were deprioritized in reduced-funding scenarios. Post-natal prophylaxis for infants and facility-based PrEP remained priorities. PrEP for pregnant and breastfeeding women remained in the at 50% scenario, driven by PEPFARs inclusion of this in their waiver. All other PrEP services, harm reduction and community condom distribution were deprioritized. | ART maintenance remained a priority. Under the 0% scenario, initiation would focus on children, pregnant/breastfeeding women, and people with advanced HIV disease (AHD).Out-of-facility activities with costs associated, including DSD models, were deprioritized.The full AHD package was deprioritized due to high cost.Viral load testing and tracking/tracing were excluded or reduced under 0% and 30% scenarios. |
Ghana
The key points and a summary Ghana’s strategic prioritization of HIV services exercise are outlined below.
Key points from Ghana’s prioritization exercise
- Decision making was guided by existing cost effectiveness analyses of specific activities.
- Commodities were considered essential and protected these from cuts.
- Projected budget savings came from adjusted systems-level activities such as supervision, DSD monitoring and training.
Ghana is considering reducing clinical visit frequency to annual for those who are established on treatment.
Summary:
- PEPFAR supports three of Ghana’s 16 regions; the Global Fund remains the principal external funder.
- Ghana initially reprogrammed its budget through exchange-rate savings and efficiencies in existing activities.
- The Global Fund reprioritization process already identified low-impact and low-uptake interventions for de-prioritization, including individual out-of-facility and community pharmacy models. Facility-based group models remain supported.
- PATHS guidance helped to engage Global Fund sub-recipients early in the prioritization process.
- Ghana used the TIER tool as a framework and adapted it to national guidance.
- Stakeholders had commodity and activity-level budgets available to guide decisions.
- They protected prevention, testing, and treatment commodities as non-negotiables.
- They reviewed the possibility of reducing systems activities to create savings, including monitoring, supervision, and training.
- They are evaluating potential savings from moving annual clinical visits to people established on treatment.
Prioritization outcomes, supported by CQUIN, using the adapted TIER tool
In the second half of 2025, the HIV Coverage, Quality and Impact Network (CQUIN), led by ICAP at Columbia University, supported the 21 member countries to complete prioritization exercises. Countries were encouraged to complete the IAS-developed TIER tool or the CQUIN-adapted TIER tool[MOU1] , prioritize monitoring and evaluation indicators, and share strategic planning meeting plans.
The CQUIN-adapted TIER tool considered what to maintain or drop under two donor-funding scenarios: 0% and 50% or higher. Costing data were not available during the exercise as countries were yet to receive confirmed funding envelopes.
A summary of outcomes from the prioritization processes of sixteen countries was presented during an August 2025 webinar (Figures 2-4). Overall, while interventions across treatment, testing and prevention were reviewed for prioritization, most countries prioritized maintaining the current HIV treatment programme (Figure 2). Some countries prioritized out-of-facility DSD models and investments in home tracing. The most commonly deprioritized testing services included recency testing and targeted outreach (Figure 3). Frequently deprioritized prevention interventions were out-of-facility activities, needle and syringe programmes and naloxone for people who use drugs (Figure 4).
Figure 2: Prioritization outcomes: Treatment
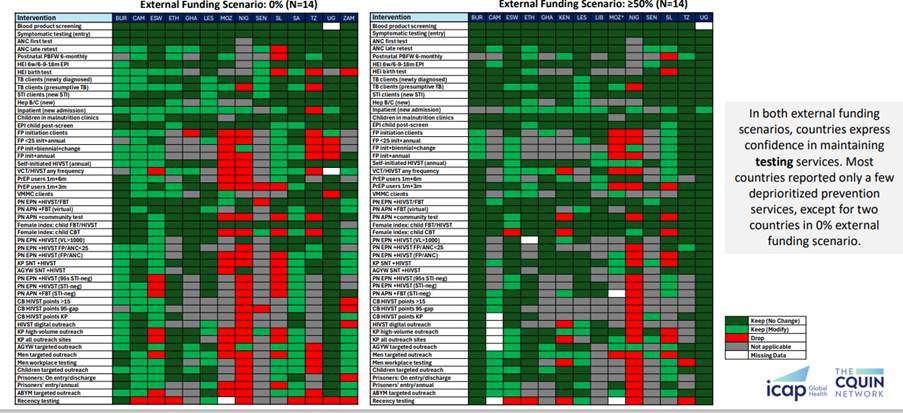
Figure 3: Prioritization outcomes: Testing
Figure 4: Prioritization outcomes: Prevention
Further details of the outcomes of country prioritization exercises are available from country presentations and posters presented at the annual CQUIN meeting.