- The PATHS - 2. "Systems" supporting HIV programmes
- 2.1 Integration of HIV services into primary care, outpatient and SRH/family planning services
- 2.2 Human resources
- 2.3 Laboratory
- 2.4 Supply chain
- 2.5 Monitoring, evaluation and quality improvement
- 2.6 Monitoring health systems elements for sustainability
- 2.7 Priority matrix for health system sustainability planning
This toolbox, developed by IAS – the International AIDS Society, together with partners, is designed as a rapidly deployable resource to support national governments in responding to unexpected reductions in HIV funding by enabling swift reassessment and reorganization of HIV systems and services.
Version: 2 July 2025



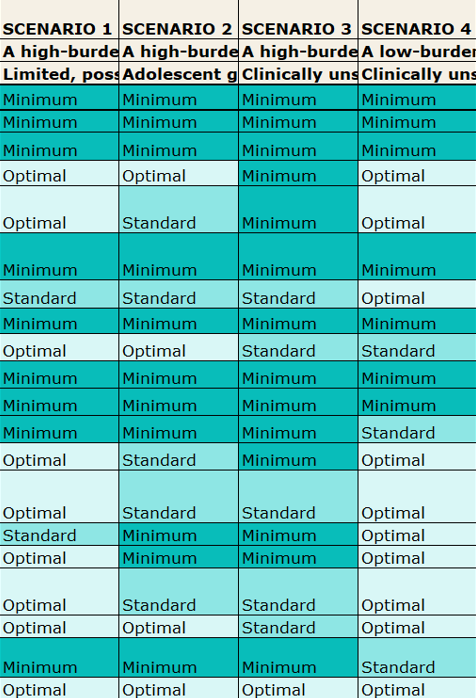
The TIER Tool – Tool for Intervention, Evaluation and Ranking (IAS) (Version 30 July 2025)
This tool offers a structured framework for prioritizing components of an HIV programme, including HIV treatment and care (continuity, monitoring, initiation and re-initiation), testing and prevention. It incorporates adaptable prioritization criteria according to the epidemiological context and progress toward the 95-95-95 targets.
French – Lʼoutil TIER dʼévaluation et de classement des interventions (IAS) (Version 30 juillet 2025)
Spanish – La herramienta de evaluación y clasificación de intervenciones (TIER) (IAS) (Versión del 30 de julio de 2025)
Portuguese – TIER – Ferramenta de Avaliação e Classificação de Intervenções (IAS) (Versão de 30 de julho de 2025)
2.1 Integration of HIV services into primary care, outpatient and SRH/family planning services
“Integration” has been considered across various healthcare services, including tuberculosis (TB), cervical cancer screening, family planning, and NCDs. Since the 2021 WHO recommendations advocating for greater integration, additional evidence has emerged – particularly regarding the integration of HIV services with chronic disease management, such as for hypertension, diabetes and mental health conditions.
Approaches to integration have included incorporating additional health services into existing vertical HIV clinics and establishing “chronic care clinics” that serve both people living with HIV and HIV-negative individuals who require life-long care medication and support for chronic conditions.
Integration into maternal and child health (MCH) services has been widely implemented for the delivery of prevention of vertical transmission interventions. WHO also recommends integrating HIV services—such as testing, prevention, and treatment—into family planning services, and vice versa. However, the implementation of family planning integration has been less widespread, particularly in terms of aligning contraceptive method refills (e.g., pills, self-injectables, and injectables) with differentiated service delivery (DSD) models for clients established on HIV treatment.
Beyond the service delivery level, integration must also be considered at the systems level. This includes human resources, laboratory networks (e.g., integrated sample transport), supply chains and monitoring and evaluation systems. These system-level considerations are explored in greater detail in this section of the toolbox.
Key questions: Integration of HIV care with other chronic conditions
- What epidemiological data are available on the mortality and morbidity impact of HIV and other chronic conditions (e.g., cardiovascular disease, hypertension, diabetes)?
- Is cascade data available for HIV, hypertension and diabetes?
- How are HIV, hypertension and diabetes services currently delivered?
- Are services delivered as vertical programmes across all levels?
- Are they vertical at district and above level hospitals, but integrated at primary care level?
- Has care for all conditions been decentralized, and if so, where?
- What model of integration has been/will be adopted?
- Have other chronic health conditions been integrated into HIV services only for people living with HIV?
- Is a chronic care clinic model being implemented (e.g., serving any client with HIV, hypertension and/or diabetes utilizing the existing HIV clinic infrastructure or with “chronic care” day or service)?
- Is HIV care being incorporated into existing outpatient department (OPD) services so that clients receive “integrated” care during their clinical visits?
- Is HIV care being integrated into broader primary health care services so that clients receive integrated” care during their clinical visits?
- Where are integrated services provided (tertiary, secondary, primary or community)? Are different approaches for integration needed at different levels?
- Who is delivering the services? Is there a need for capacity building of human resources across disciplines (clinical, M & E, pharmacy, laboratory) for any of the disease areas?
- Are there clear criteria to define clients with chronic conditions as being established on treatment?
- When are services provided? Are there clear criteria for the frequency of clinical visits and the duration of medication refills?
- Is multi-month prescribing (MMP) practiced across chronic conditions?
- Is MPP coordinated across different services?
- Is there capacity for multi-month dispensing (MMD) across chronic conditions?
- Are medications for other conditions available free of charge?
- Do people pay out of pocket for chronic care medications?
- Are medications covered by national health insurance schemes?
- Are there plans to integrate HIV medications into national health insurance coverage?
- Are diagnostic and monitoring investigations for chronic conditions provided free of charge?
- Are they included in national health insurance schemes?
- Are there plans to include HIV diagnostics and monitoring in national health insurance schemes?
- If not already integrated, should laboratory, supply chains and monitoring and evaluation systems be integrated?
(These topics will be discussed in more detail in the following sections)
Tools and resources for hypertension and diabetes integration
INTE-AFRICA Study
Evidence for an integrated model of HIV, hypertension and diabetes care
More information on the INTE-AFRICA Study
The INTE-Africa study evaluated a fully integrated model of HIV, hypertension, and diabetes care in sub-Saharan Africa, including participants with chronic conditions who did not have HIV. This large, randomized study was conducted in two countries- Tanzania and Uganda- and followed more than 6,000 participants attending 32 health facilities for 12 months.
The key findings were that integrated management resulted in high rates of retention in care for people with diabetes, hypertension, or both. Viral suppression rates were not adversely affected, and the integrated model was cost-saving for health services.
The cost results showed the mean monthly service cost managing two conditions in a single individual was: $39.11 (95% confidence interval (CI): 33.99, 44.33) for HIV and diabetes, $32.18 (95% CI: 30.35,34.07) for HIV and hypertension and $22.65 (95% CI: 21.86, 23.43) for diabetes and hypertension. These costs were 34.4% (95% CI: 17.9%, 41.9%) lower than managing any two conditions separately in two different people. Managing all three conditions in a single individual was 48.8% (95% CI: 42.1%, 55.3%) cheaper than managing them separately. Out-of-pocket expenditure per participant per visit was $7.33 (95% CI: 3.70, 15.86), representing 23.4% (95% CI: 9.9, 54.3) of the total monthly service expenditure per participants and 11.7% (95% CI: 7.3, 22.1) of their individual total household income.
DSD for chronic conditions. A supplement to A Decision Framework for antiretroviral therapy delivery
IAS – the International AIDS Society, 2024
More information on DSD for chronic conditions. A supplement to A Decision Framework for antiretroviral therapy delivery
This framework outlines how the principles of DSD can be applied across chronic conditions. Key components include defining criteria for “established on treatment”, WHO guidance and evidence on the frequency of clinical visits, support for task-sharing and case examples of integration and chronic disease DSD models.
Integrating Hypertension and HIV Toolkit: A Practical Differentiated Service Delivery toolkit
Resolve to Save Lives, 2023
More information on Integrating Hypertension and HIV Toolkit: A Practical Differentiated Service Delivery toolkit
This practical toolkit demonstrates how DSD principles can be adapted for chronic diseases, particularly hypertension. It includes example standard operating procedures (SOPs) for each of the four DSD models and tools and templates to support programme design and implementation.
Country experiences with hypertension and diabetes integration
South Africa
South Africa’s national DSD guidance has, for many years, included all chronic conditions, with a particular focus on hypertension and diabetes. Key features of the guidance include definitions of “established on treatment” across chronic conditions and SOPs for all the DSD models for all chronic diseases.
Uganda
In quarter 1 of 2025, the Uganda ministry of Health initiated a nationwide acceleration towards integration in response to donor funding cuts. A National Advisory Committee on Integration (NACI) has been established overseeing the development of implementation plans for service delivery, human resources for health, financing, supply chain and data and health information systems.
Resources:
- Uganda integration planning overview slides (Slides 39-60)
- Terms of Reference (ToR): Integration consultant
- Terms of Reference (ToR): national advisory committee (NACI)
- Integration support supervision tool
- Tools being developed by CHAI to support capacity building
Key questions for integration of HIV care and family planning
- What is the current epidemiological and service delivery context for HIV and family planning?
- What are the rates of unintended pregnancy and contraceptive use?
- What are the rates of unintended pregnancy and contraceptive use among women living with HIV?
- What are the HIV prevalence and incidence trends among women of reproductive age?
- How are HIV and family planning services currently delivered?
- Are family planning services integrated into HIV treatment and care for people living with HIV?
- Is HIV testing, prevention (e.g., PrEP), and treatment integrated into family planning service platforms?
- Are services for the prevention of vertical transmission routinely delivered within antenatal and postnatal care for mothers and HIV-exposed infants?
- What model of integration has been/will be adopted?
- Are contraceptive services and refills co-delivered at the same differentiated service delivery (DSD) distribution points as ART?
- Are the durations of contraceptive refills aligned with ART refill schedules (e.g., multi-month dispensing)?
- Are women already enrolled in DSD models supported to remain in their model during and after pregnancy?
- Are tailored DSD models available for pregnant and postpartum women in antenatal and postnatal services?
- Where are integrated services provided?
- Are integration efforts implemented at tertiary, secondary, primary, or community levels implemented?
- Are different models required at different levels of the health system?
- Who is delivering the services?
- Are healthcare workers cross-trained to provide both HIV and family planning services?
- Are there team-based or task-sharing approaches in place to support integration?
- What family planning methods are available and accessible in HIV service settings?
- Is a full range of contraceptive options provided, including short- and long-acting methods?
- Are method refills (e.g., pills, injectables, self-injectables) aligned with HIV DSD models?
- Is access equitable and affordable?
- Are contraceptives and HIV services provided free of charge in integrated settings?
- Are services covered by national health insurance schemes?
- Are user fees or stockouts limiting access to either service?
- Are client rights and preferences respected?
- Are women and adolescents offered non-coercive, rights-based counselling on reproductive options?
- Are key populations able to access integrated services without stigma or discrimination?
- Are monitoring, supply chain and data systems coordinated?
- Can contraceptives and HIV commodities be managed within a shared supply chain system?
- Are information systems integrated to capture service utilization and outcomes for both FP and HIV?
- Are joint indicators used for monitoring the effectiveness of integration efforts?
Tools and resources for family planning integration
Differentiated service delivery for family planning services and contraceptive methods including opportunities for integration of ART and PrEP
IAS, 2025
More information on Differentiated service delivery for family planning services and contraceptive methods including opportunities for integration of ART and PrEP
This supplement to A Decision Framework for antiretroviral therapy delivery outlines how DSD models can be leveraged towards strengthening family planning services including through integrated DSD for HIV treatment and PrEP.
Resources from the WHO
The resources from WHO provide a range of guidance on the integration of family planning services for people living with HIV and comprehensive implementation guidance for attaining triple elimination of HIV, Hepatitis B and syphilis through the provision of prevention services at antenatal, delivery and postnatal services.
- SRHR & LINKAGES TOOLKIT
- Integration of HIV testing and linkage in family planning and contraception services: implementation brief, WHO, October 2021
- Actions for improved clinical and prevention services and choices: preventing HIV and other sexually transmitted infections among women and girls using contraceptive services in contexts with high HIV incidence, WHO, June 2020
Country examples of family planning integration
The following documents provide country examples of SRH and HIV integration policies.
Implementation Guide for the National Strategy for Integration of Sexual Reproductive Health and Rights and HIV/AIDS 2017-2021
Uganda Ministry of Health, 2017
Tools and resources for integration
Technical Brief: Integration of noncommunicable diseases into HIV service packages
WHO, 2023
Integrating the prevention and control of noncommunicable diseases in HIV/AIDS, tuberculosis, and sexual and reproductive health programmes: implementation guidance
WHO, 2023
More information on Technical Brief: Integration of noncommunicable diseases into HIV service packages, and Integrating the prevention and control of noncommunicable diseases in HIV/AIDS, tuberculosis, and sexual and reproductive health programmes: implementation guidance
These guidance documents from WHO provide practical implementation guidance for integration of NCDs and HIV services. The guidance is designed to facilitate the implementation of WHO integrated, people-centred health services placing primary care and essential health functions at the core of integrated health services. They provide pragmatic, holistic solutions, such as evidence-based checklists, practical considerations, case studies and tools for various stakeholders.
The documents consider the importance of multisectoral policy, empowering people and communities, avoiding fragmentation of health systems and ensuring better coordination and collaboration with organisations and providers in all care settings.
Integrating HIV programs into primary health care systems: Practical considerations for county decision makers
Genesis Analytics (Pty) Ltd, 2024
More information on Integrating HIV programs into primary health care systems: Practical considerations for county decision makers
This document presents a flexible pathway for integrating HIV services into PHC systems – or integrating other health services into HIV programmes. It provides detailed step-by-step considerations to guide the Ministries of Health and Finance, HIV and PHC programme managers, implementing partners and donors. The approach emphasizes the need for responsive, context-specific implementation strategies tailored to country-specific settings and addressing integration at service delivery, systems, financing and governance levels to underpin successful scale-up of integration efforts.
More information on Literature database for HIV service integration
This user-friendly dashboard is a consolidated database of 170 studies examining pathways to HIV integration. The “consolidated database” sheet offers a collection of literature on HIV service integration. There are also specialized sections on “costing literature” and “cost effectiveness”.
Integration Primer – Pragmatic Considerations for Advancing Integrated Systems and Services for Strengthened Primary Health Care
PATH, January 2026 (updated version)
More information on Integration Primer – Pragmatic Considerations for Advancing Integrated Systems and Services for Strengthened Primary Health Care
This refreshed primer aims to equip policymakers, health system planners, implementers, advocates, and donors with pragmatic guidance, learnings, and tools as they advance integrated systems and services to strengthen PHC.
Readiness Assessment and Prioritization for Integration Decisions (RAPID)
PATH, January 2026
More information on Readiness Assessment and Prioritization for Integration Decisions (RAPID)
The Readiness Assessment and Priorization for Integration Decisions (RAPID) tool is designed to support sub-national health manager and planners. It provides a structured approach to assessing the current state of integrated services and systems at the PHC level, including the degree of integration- from relatively limited to advanced – and to identify priority actions to strengthen integration. The RAPID tool is not intended to produce a pass/fail score for integration. Rather, it supports evidence-informed planning, coordination and prioiritzation to advance integrated services and systems.
2.2 Human resources
Building the capacity of human resources to deliver HIV services – and embracing the principle of task sharing – has been fundamental to the scale-up of ART. In many settings, additional cadres paid by implementing partners are not formally included in Ministry of Health workforce planning. As funding reductions continue, there will likely be a substantial impact on the availability, distribution and sustainability of the HIV workforce.
Considering this, the following key questions are offered in the grid below (Table 2) for consideration at each level of human resources involved in the coordination and delivery of HIV services.
Key questions
Table 2: HR for HIV services assessment grid – to be adapted to context.
Downloadable editable table
| Management and coordination of programme | Clinicians (Doctors, clinical officers, nurses) | Community Health Workers | Peers | Monitoring & Evaluation Staff | Laboratory Staff | Pharmacy Staff | |
|---|---|---|---|---|---|---|---|
| 1 | Has a mapping of the cadres’ full-time equivalent positions at national, provincial and district levels been conducted? | ||||||
| 2 | How many of these positions are funded by donors or partners? | ||||||
| 3 | Are current roles aligned with the delivery of minimum, standard and optimal service packages? | ||||||
| 4 | What opportunities exist to adapt roles to support integrated services beyond HIV? | ||||||
| 5 | How are these HR roles addressed (inclusion, numbers) in the national human resources strategy? | ||||||
| 6 | What plans are in place for the continuing education, mentorship and leadership development of each cadre? | ||||||
2.3 Laboratory
Key questions
- Is there a plan in place for the ongoing service, maintenance, and calibration of HIV-related laboratory equipment? How will these services be funded?
- What quality assurance systems exist for HIV-related laboratory testing? Is there a plan for sustaining quality assurance activities, and how will they be financed?
- Given current or anticipated budget constraints, is there a need to revise clinical guidelines on the frequency of HIV-related tests (e.g., viral load monitoring)?
- Should existing HIV testing algorithms be re-evaluated in light of current 95-95-95 status and changing resources? What are the implications for service delivery?
- How is sample transport currently organized and funded? What changes, if any, are anticipated due to shifting donor support?
- If not already in place, is there an opportunity to implement or strengthen an integrated sample transport system across programmes?
- Are additional systems in place for result delivery (e.g., SMS-based notifications)? How are these systems currently funded, and are they financially and operationally sustainable?
Tools and resources
The following resources provide examples and best practices related to integrated sample transport systems, including establishing a hub and spoke model. Strategies related to organization and management, implementation and ensuring quality assurance of sample handling are also provided. The example from Nigeria demonstrates the use of third-party logistics providers to establish a national integrated sample transport system.
LabCoP Cookbook of best practices: Recipe #1: Sample transport system
African Society of Laboratory Medicine, 2019
Integrated sample transportation system (IST) concept note
Zimbabwe Ministry of Health and Child Care
2.4 Supply chain
Key questions
- Who currently coordinates and funds procurement processes?
- What human resources are required to support procurement, and who funds these positions?
- Is high-quality, timely data available to support accurate forecasting of diagnostic and medication needs?
- Who is responsible for coordinating and funding the overall supply chain system?
- What human resources are needed for supply chain operations, and how are they funded?
- Is funding available for the maintenance and upgrading of information systems that support procurement and supply chain management?
- What warehousing systems are in place, and who is responsible for funding them?
- Are forecasting and supply chain systems for HIV commodities managed as vertical programmes or integrated within broader systems? Is there an opportunity for integration, and would it be more cost-effective or efficient?
Tools and resources
More information on Ghana health supply chain master plan 2025-2029
The Ghana Health Supply Chain Master Plan describes the development of an integrated supply chain system aligned with the goal of achieving Universal Health Coverage. The domains considered in the plan include strategic planning and management, forecasting and supply planning, procurement and customs clearance, distribution, quality and pharmacovigilance and healthcare waste management.
2.5 Monitoring, evaluation and quality improvement
Key questions
Indicator package and data use
- What package of indicators is currently used by the national programme for HIV prevention, testing and treatment?
- Is there a need to adapt or simplify the current indicator set?
- Should the indicator set be revised to align with the minimum, standard and optimal service delivery packages?
- Is there a plan to transition to sentinel sites or other targeted methods for individual-level data analysis?
Information systems
- What strategic information systems are currently in use for monitoring and evaluation?
- Has a national M&E tool been selected and endorsed?
- Who funds the development, maintenance and infrastructure (hardware and software) of the national M&E system?
- Is the current national M&E system for HIV inclusive of other chronic conditions, or limited to HIV?
- Are there opportunities to support the development of an integrated national monitoring and evaluation platform that includes HIV and other chronic conditions?
Data use and feedback
- How is data currently analyzed, visualized, and shared with managers and service providers?
- To what extent is this data analysis and feedback process reliant on donor support?
Quality improvement (QI)
- What quality improvement programmes are currently established within the national HIV response?
- How are these QI programmes funded, and are there examples of successful implementation that could be shared (e.g., Kenya)?
Community-led monitoring (CLM)
- What community-led monitoring activities have been funded in the past financial year?
- What are the opportunities and requirements to sustain or expand community-led monitoring efforts?
Note: Human resources for monitoring and evaluation are addressed in Section 2.2.
Country experience
Kenya: Moving towards an integrated strategic information system for chronic conditions.
Kenya has selected a single health information system to support cohort monitoring of patients with HIV, hypertension and diabetes. A summary presentation on this can be found here.
2.6 Monitoring health systems elements for sustainability
In addition to adapting monitoring tools that track clinical outcomes, it is essential to monitor the implementation of the sustainability plan across the various pillars of the health system, especially as health systems adjust to significant funding shifts. The resources in this section offer a framework for selecting health systems metrics to track both the actions taken and the effectiveness of changes made in delivering HIV programming.
Tools and resources
Two tools from Genesis Analytics aim to support monitoring and evaluation of the systems components within an HIV program and/or national response and provide non-prescriptive direction for selecting suitable indicators to monitor and measure progress towards strengthened public primary health care systems.
Selecting Health Systems Metrics for HIV Response Sustainability Planning
Genesis Analytics, July 2024
Health Metrics Database for Sustainability Planning
Genesis Analytics, September
2023
More information on Selecting Health Systems Metrics for HIV Response Sustainability Planning, and Health Metrics Database for Sustainability Planning, Genesis Analytics
The tools recommend a limited set of the most suitable and high-quality indicators that can be used to track progress towards goals. The recommended indicators are framed within an easy-to-use typology that organizes the indicators by health system sub-domain and by generic sustainability goal statements for those sub-domains.
Stakeholders are encouraged to consider the array of recommended health systems indicators in this reference and select the most appropriate indicators to suit their country’s context.
For each indicator, a brief rationale is provided to assist with the selection process. The suitability of each indicator for various country contexts is also provided, again to support stakeholders with selection.
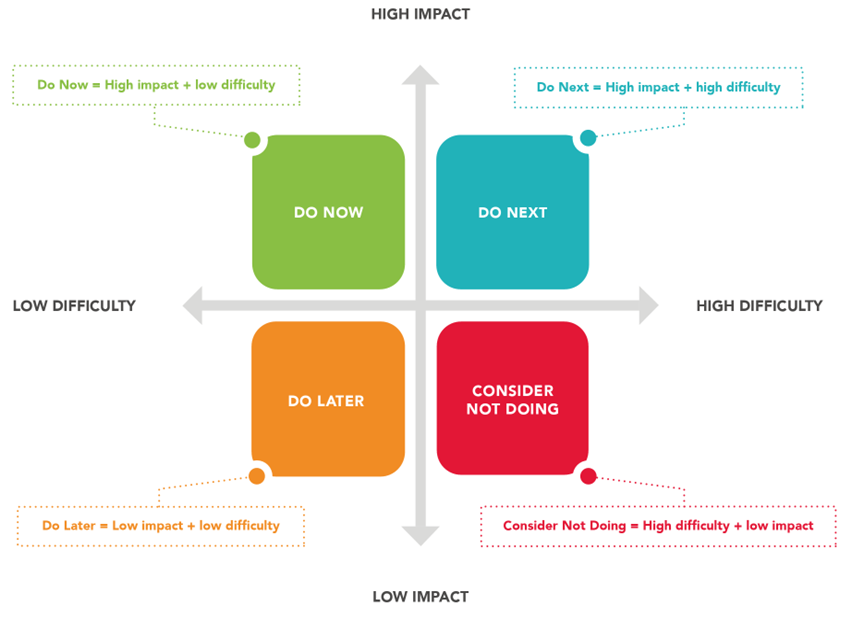
2.7 Priority matrix for health system sustainability planning
For each area of health system planning, multiple actions may need to be implemented and monitored. Once an action plan has been developed for each health system pillar, the priority matrix can be used to sequence and prioritize these actions (Figure 2). The primary goal of this tool is to identify and fast-track actions that are high-impact, feasible to implement, and require minimal investment—ensuring they are prioritized for immediate execution.
Figure 2: The priority matrix