
Five-step approach
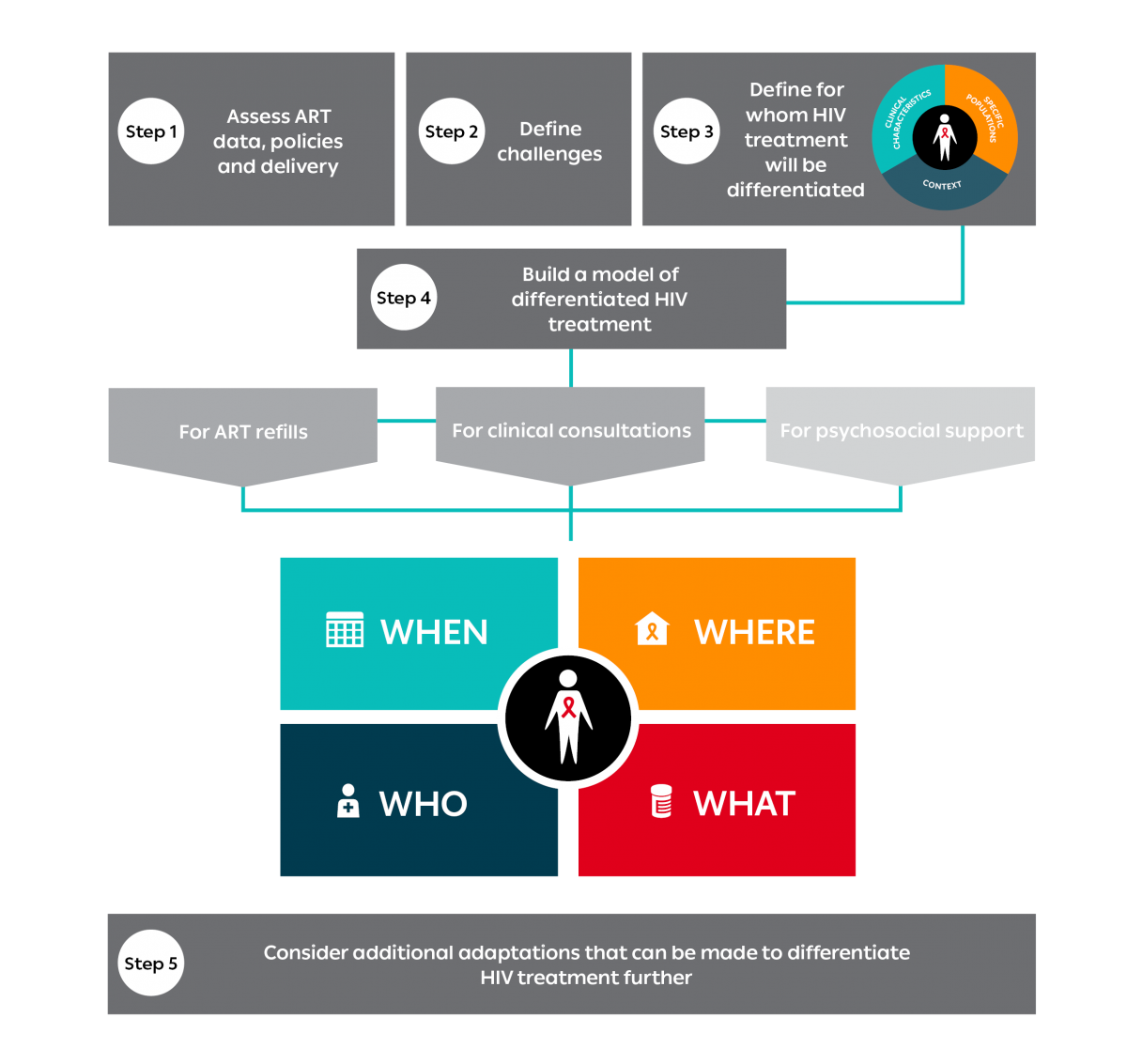
The five-step approach guides ministries of health, supporting partners and communities in planning how to differentiate HIV treatment services (antiretroviral therapy delivery):
To support this process, several annexes are available for download here.
STEP 1: ASSESS ART DATA, POLICIES AND DELIVERY
Before you begin, it is important to assess the current situation.
Assess the current situation by downloading the facility-level questionnaire (Annex 2) and the template for assessing relevant policies (Annex 3) here. Then complete the following three assessments:
1.1 Assess the data
Routine monitoring and evaluation (M&E) data on retention helps determine what the challenges are at the site level. Relevant data includes the number of people on antiretroviral therapy (ART) and retention data for specific sub-populations. It is also important to know if facilities have an appointment and tracing system.
Complete Section 1 of the facility-level questionnaire (Annex 2) to conduct your baseline assessment.
1.2 Assess the policies
A comparison of national-level policies with current World Health Organization (WHO) recommendations may also be undertaken. Policies should be reviewed in alignment with the building blocks (Step 4) and to support HIV treatment delivery in general. Use the template for assessing the relevant policies.
1.3 Assess the current models of HIV treatment delivery
An initial broad mapping of differentiated HIV treatment delivery is recommended to determine what is being implemented in-country and the current coverage of the models. Using the building blocks (Step 4) and the elements (Step 3) as helpful tools, your mapping may be carried out through a desk review of published literature and local country and partner activity reports in combination with a survey of district ART coordinators and implementing partners.
Complete Section 2 of the facility-level questionnaire (Annex 2) to help conduct your mapping.
STEP 2: DEFINE CHALLENGES
Identify the challenges that can be addressed through differentiated HIV treatment delivery.
Based on Step 1, you should now be able to identify the challenges that can be addressed through DSD for HIV treatment. However, you will also want to assess the healthcare worker and client perspectives to understand their challenges, as well as preferences and expectations.
At this stage, it is important to host a workshop and engage key stakeholders from both the health system and civil society to achieve the following objectives:
- Sensitize ART coordinators and implementing partners on the background and core principles of differentiated HIV treatment delivery.
- Provide an opportunity for stakeholders to present existing examples of differentiated service delivery models implemented in their settings.
- Present the outcomes of the national-level desk review.
- Summarize the findings from the consultations with healthcare workers and people living with HIV.
- Engage stakeholders in a plan for local or district situation analysis.
Complete Sections 3 and 4 of the facility-level questionnaire (Annex 2) to add their perspectives.
STEP 3: DEFINE THE POPULATION(S) FOR WHOM ART DELIVERY WILL BE DIFFERENTIATED
Consider the three elements: clinical characteristics, sub-population and context.
You are now ready to proceed with prioritizing differentiated HIV treatment delivery. The three elements will assist you in building appropriate models as described in Step 4.
To learn how to differentiate based on clinical characteristics, specific population or context, see the three elements from page 13.
STEP 4: BUILD A MODEL OF DIFFERENTIATED HIV TREATMENT DELIVERY
The building blocks are the key components of a service delivery model.
Once you have defined who is eligible, you can proceed with building a model of differentiated HIV treatment delivery.
In addition to the elements from Step 3, use your completed facility-level questionnaire from Step 1 to assist you.
The building blocks of differentiated HIV treatment delivery centre on four questions: “when”, “where”, “who” and “what”. These build the foundation of a differentiated model of service delivery.
In all models of ART delivery, the client is at the centre. It is up to the district health manager to work with healthcare workers and clients to determine how to address each the “when”, “where”, “who” and “what” blocks in the DSD model. The stakeholders must balance the goal of improving client outcomes with their ability to utilize the available health system resources.
Models for clients who are established on ART
Recent innovations in ART delivery, or DSD for HIV treatment for clients who are established on ART, can be categorized into four models.

Health care worker-managed groups
Clients receive their ART refills in a group and either a professional or a lay health care staff member manages this group. The groups meet within and/or outside of health care facilities.

Client-managed groups
Clients receive their ART refills in a group but this group is managed and run by clients themselves. Generally, client-managed groups meet outside of health care facilities.

Facility-based individual models
ART refill visits are separated from clinical consultations. When clients have an ART refill visit, they bypass any clinical staff or adherence support and proceed directly to receive their medication.

Out-of-facility individual models
ART refills and, in some cases, clinical consultations are provided to individuals outside of health care facilities.
Within these models, all clients continue to have clinical consultations as part of their package of care. Multiple models can work in parallel so that a client can move between them in the course of their lifetime. Further, the models are flexible to accommodate clients who may want to be up referred or require up referral. By being up referred, the intensity of care is increased to reflect the increased clinical needs of the client.
FAQ
Antiretroviral therapy (ART) supply
If longer refills are not available through national supply, does this mean we cannot differentiate ART delivery?
No. A current inability to provide longer refills should not be a barrier to differentiating ART delivery following the building blocks and elements approach. In fact, it was having access to only a one-month supply of ART that drove clients in Mozambique to develop community ART groups.
However, without a secure supply of ART, the potential gains of differentiating ART delivery may not be maximized. Strengthening of forecasting, procurement and supply chain requires ongoing investments.
Does delivering ART to the community compromise drug security?
No. To date, in the countries where ART delivery has been differentiated into communities, there have been no documented or reported incidences of drugs not arriving, going missing or being stolen.
There are a number of steps that can be taken to avoid incorrect distribution or loss of drugs:
- Community leaders and community-based organizations representing people living with HIV (PLHIV) should be consulted and involved in the programme from its inception.
- All PLHIV receiving their ART through out-of-facility models should understand their regimen and know the name of their regimen and what the packaging for their formulation looks like.
- Prior to community distribution of ART, all drugs should be pre-packed at the facility.
- Dispensing of ART should be monitored within the standardized M&E system and any non-collection of ART should be reported to the facility.
Access to routine viral load monitoring
Can ART delivery be differentiated in settings with limited or no routine viral load monitoring?
Yes. Although viral load monitoring facilitates differentiation of ART delivery by providing a quantitative assessment of treatment success, its absence should not be a barrier to differentiating care. Many models of differentiated service delivery were established prior to the availability of viral load testing. Definitions of “established on ART” can be made as per the WHO recommendations using either immunological or clinical criteria.
However, access to viral load monitoring can reassure both the clinician and the client that ART is working effectively and provides a more solid foundation for moving forward with client self-management, reducing frequency of visits and moving to ART distribution in the community.
How does access to routine viral load support differentiating ART delivery?
Scale up of viral load testing has primarily been seen as an intervention to identify treatment failure early and switch clients appropriately to second-line treatment. Using viral load to identify clients who are established on ART and who may be able to be seen less frequently and in the community is an important outcome of routine viral load testing. Routine viral load monitoring can be cost effective if clients who are virally suppressed receive differentiated ART delivery based on the result. With a suppressed viral load, clinicians have an objective measure of treatment success that can support less frequent clinical consultations. Reducing clinical consultations to every 12 months for clients who are virally suppressed should be considered with access to routine viral load monitoring.
Viral suppression outcomes and costing evidence
Are there viral suppression data for differentiated ART delivery models?
Yes, there are viral suppression outcome data for differentiated ART delivery models. Currently, studies reporting viral suppression evaluate ART adherence clubs (a health care worker-managed group model) and streamlined HIV care (a facility-based individual model). A 2016 analysis of a cluster random sample of 10% of all clients in ART adherence clubs reported viral suppression of 96.8% (CI 96-97.4) at 12 months and 96% (CI 95-97) at 24 months after enrolment in a club. Viral suppression outcomes from pilots in Uganda and Kenya were 89% for adults 12 months after enrolment in streamlined care from ART start (at first visit), and 92% for children 48 weeks after enrolment. For further viral suppression data, see the summary of evidence related to these two models of care (health care worker-managed groups, facility-based individual models).
Are there costing data for differentiated ART delivery models?
Yes, there are costing data across a range of differentiated ART delivery models. From out-of-facility ART delivery models, there is costing of home ART delivery and a cost comparison of the The AIDS Support Organization (TASO) model (which includes fixed community distribution points with mobile ART delivery and nurse-led facility-based care in Uganda). For facility-based individual models, pharmacy-only pick-up in Uganda and streamlined care in Uganda and Kenya have been costed. In health care worker-managed groups, the ART adherence club has been costed, and a scaled implementation costing was included in the South African HIV and TB Investment Case. For more details, see the summary of evidence related to these models of care.
Achieving optimal differentiated ART delivery implementation
Once a country has adopted a differentiated ART delivery policy, what should be done next?
Implementation support from national to district level and from district level to facilities is required to support the assessment process for which model/s are suitable for implementation at each facility. Once facilities have decided on their model/s, they may require implementation guidance and/or support from district level. Where facility implementation is slow, district quarterly target setting for enrolment into model/s has been shown to work. Ongoing monitoring of facility enrolment at district and national level is useful to assess implementation progress and to direct where active support may be needed. Further, people living with HIV can support scale-up by requesting a differentiated ART delivery model based on what is recommended in the national policy.
Differentiated ART delivery in low-prevalence settings
Can a low HIV-prevalence setting benefit from implementing differentiated ART delivery?
Yes. The main purpose of differentiating ART delivery is to better provide for the client’s specific needs at a particular point along their continuum of care. However, client needs must be balanced against what it feasible for the health system based on its context. In a low-prevalence setting, it may not be feasible to train all health providers to manage HIV in order to provide clinical care close to the client’s home. A possible alternative approach would be to continue centralizing HIV clinical care, but reducing the frequency of clinical review (once or twice a year) and providing ART refills closer to home at clinics and community pharmacies or by home delivery.
Differentiated ART delivery for key populations
How can differentiated ART delivery improve treatment outcomes for key populations?
Key populations are disproportionately affected by HIV, but under-represented in HIV treatment programmes. This is partly due to stigma and discrimination experienced when accessing facility-based services. Treatment outcomes may be improved by reducing the frequency of clinical review visits and facilitating ART refill collection within key population communities or at community sites where key population members feel comfortable. Task shifting ART refill visits to key population peers can increase involvement of key population communities and organizations and also support improved outcomes.
Is there WHO guidance for differentiated ART delivery for key populations?
Yes, there is. In July 2017, WHO (in collaboration with IAS, PEPFAR, CDC and USAID) released the Key considerations for differentiated antiretroviral therapy delivery for specific populations: children, adolescents, pregnant and breastfeeding women and key populations advocating and giving rationale for provision of differentiated ART delivery for these populations.
Differentiated ART delivery for children, adolescents and pregnant and breastfeeding women and their exposed infants
Do children who are established on ART require more frequent clinical monitoring than their adult counterparts?
Yes, younger children (less than 5 years of age) require more frequent monitoring. For younger children who are established on ART, 3-monthly clinical reviews are appropriate. ART refills are ideally provided for the full 3 months and collected at the clinical review visit. However, for older children (ages 5-10 years), clinical monitoring can be at the same frequency as adults who are established on ART. Weight changes leading to required dosage adjustment for older children become infrequent and these can be identified and managed at 6-monthly clinical review visits with 3-6 monthly ART refills. Where 3-monthly ART refills are provided, these should be as close to home as possible, either in communities or at the closest clinic (even if this clinic is not the location of clinical review visits).
Should all adolescent differentiated ART delivery models include peer interaction environments?
Peer environments support treatment adherence during adolescence. However, it is not always feasible to offer peer environments, such as support groups, especially in contexts with low concentrations of adolescents. Further, peer environments may not benefit all adolescents. It is important to consider that adolescents who are established on ART have already demonstrated their adherence to their treatment (e.g., suppressed viral load and/or evidence of adherence). They should therefore have access to differentiated ART delivery (less frequent clinical review visits, longer ART refills, closer to home) even where peer support is not provided. It is important that effective referral systems are put in place to pick up changes in psychosocial, mental health or sexual reproductive health needs that require attention. Other options to consider for adolescents are the peer support possibilities offered by the virtual environment.
Should women already accessing differentiated ART delivery at conception be removed from their ART delivery model and receive integrated care within antenatal services?
No, women accessing differentiated ART delivery at conception should be given the choice on how to receive their HIV care (and ART refills) during pregnancy and post-partum. If a woman remains clinically stable during her pregnancy (i.e., undetectable viral load) and prefers to continue receiving her HIV care and ART refill through her differentiated ART delivery model, she should be able to do so and access her antenatal care in parallel. It is possible to incorporate within both the clinical review and ART refills visits a check-in to ensure that the pregnant woman is attending her antenatal care. It may also be possible to incorporate the pregnant woman’s HIV care within her antenatal care, but also allow her to continue collecting her ART refill as she was before.
Should women who start ART during pregnancy be eligible for differentiated ART delivery during breastfeeding?
Yes, it will make it easier to continue treatment at an already challenging time when frequent infant follow-up health visits place even more demand on a new mother. During the post-partum period, women initiated on ART during pregnancy may become eligible for differentiated ART delivery once she meets the “established on ART” criteria. In addition, post-partum women should have more frequent viral loads than her non-pregnant adult counterparts – twice yearly rather than once yearly – until her baby has reached 18 months of age and is confirmed to be HIV negative.
Is there WHO guidance for differentiated ART delivery for children, adolescents, pregnant and breastfeeding women?
Yes, there is. In July 2017, WHO (in collaboration with IAS, PEPFAR, CDC and USAID) released the Key considerations for differentiated antiretroviral therapy delivery for specific populations: children, adolescents, pregnant and breastfeeding women and key populations advocating and giving rationale for provision of differentiated ART delivery for these populations.
Is there evidence reporting good retention and viral suppression outcomes for children, adolescents and pregnant and breastfeeding women receiving their care through differentiated ART delivery models?
Yes, there is, but it is fairly limited. Cohort analyses have reported outcomes for family and youth club (health care worker-managed group models) pilots from Khayelitsha, Cape Town, South Africa, and streamlined HIV care (facility-based individual model) for children aged 2-14 years in study sites in Uganda and Kenya. For a full list of evidence, including grey literature, see the background review undertaken in preparation for WHO November 2016 consultation on differentiated service delivery for children, adolescents, pregnant and breastfeeding women and key populations.
Framework documents
Download the Framework
Click here to access the complete DSD framework for HIV treatment services (antiretroviral therapy delivery)