
By Lana Lee (USAID), Jessica Stephens (USAID), and Catherine Godfrey (Office of the Global Health Coordinator, United States)
With more robust and better-tolerated dolutegravir-based antiretroviral (ARV) regimens now widely available, achieving the third 95 target on viral suppression should be within reach, provided HIV treatment programmes can ensure continuity of treatment for all people living with HIV. Treatment interruptions can lead to a loss of virological control, which has profound implications for people on HIV treatment. There is a growing body of scholarship implicating even low-level viremia with adverse treatment outcomes, including mortality.
Treatment interruptions are common for many chronic conditions, including HIV, and the US President’s Emergency Plan for AIDS Relief (PEPFAR) has begun evaluating programme-level data on treatment interruptions, hoping to determine factors that may help identify individuals at risk for interruption. PEPFAR defines a treatment interruption as no clinical contact or ARV pick-up for greater than 28 days since a client’s last expected clinical contact or ARV pick-up. These information is disaggregated to include those who interrupt within three months and those who have dropped out of care for more than a year. Treatment re-engagement, however, is important, and it may be that the side-by-side analysis of these two distinct entities points to areas for further study.
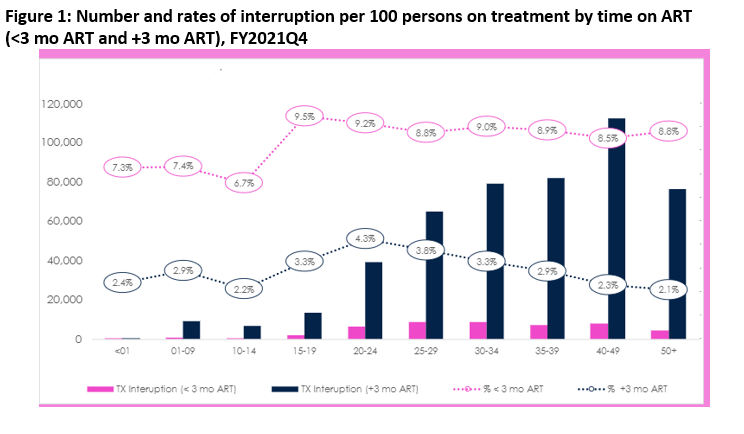
Evaluation of treatment interruptions in PEPFAR globally provides some information about who interrupts treatment and when. Data from FY2021 shows that the percentage of individuals who drop out of care within the first three months of therapy is considerably higher than those who drop out later in care and that this percentage in 2021 is consistent across all adult age groups (see Figure 1, PEPFAR data 2021). It is important to note that the absolute numbers of individuals who interrupt treatment are higher among those who are established on treatment.
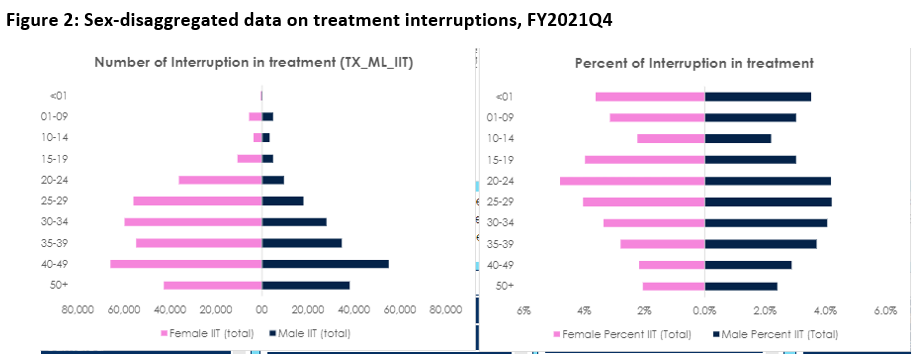
Similarly, disaggregating data by sex may be helpful. There are many more women in care, but looking at the interruptions as a percentage of those in care shows that men are at higher risk for treatment interruption (Figure 2, data from FY2021Q4).
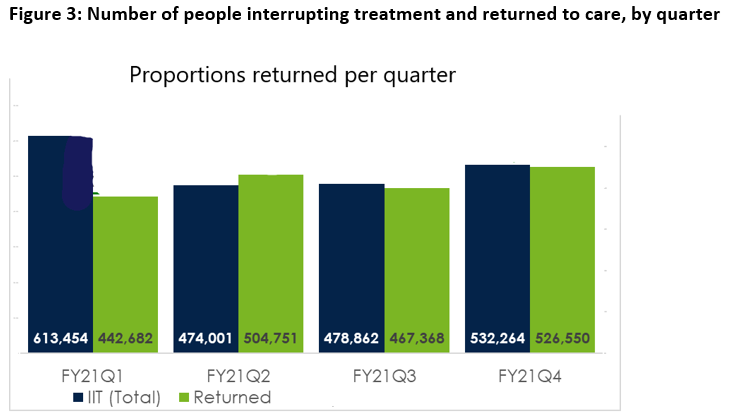
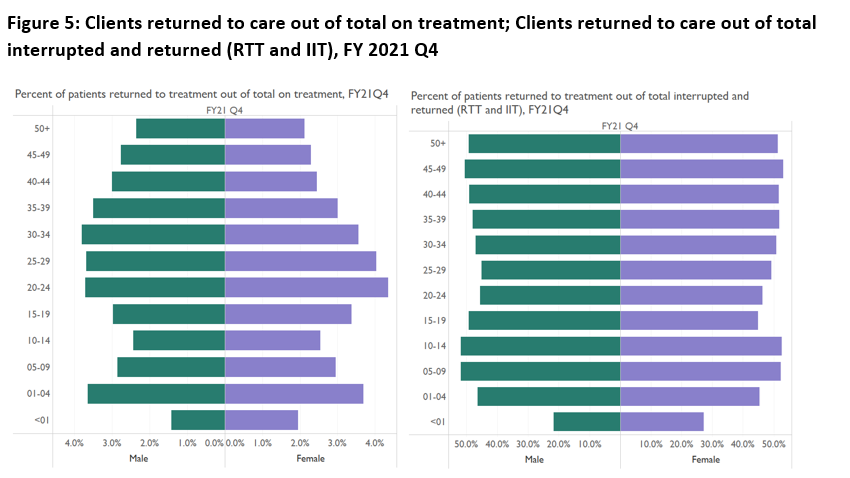
PEPFAR has recently begun collecting data on individuals who return to care. Overall, the numbers of individuals returning to care were similar to those interrupting treatment (Figure 3, data from FY 2021).
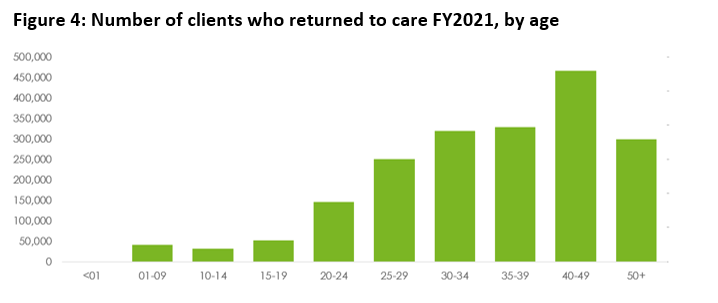
Evaluating this information by sex suggests that women return more commonly and that age disaggregations may help identify age periods when returns are more likely.
The major caveat with these data is that the data on individuals who are returned to treatment do not represent the same people who interrupted treatment, so no client-level inferences may be made from aggregate programme statistics. However, these new programme metrics may help us better understand who may interrupt treatment more commonly and may help us understand some of the broader motivators for re-engagement. Further, longitudinal client records in national public health data systems will be vital in assessing risk and refining approaches that will prevent interruptions in treatment and promote successful re-engagement.
Declaration: The authors declare no conflicts of interest.
Disclaimer: The views in this article are those of the authors and do not necessarily represent the views of USAID, PEPFAR, or the United States Government.